
Patients whose immune responses are suppressed, immunocompromised, frequently suffer from recurrent HSV infections that are much more painful than infections in immunocompetent patients. The recurrences are mostly caused by reactivation of a latent infection that was acquired prior to the period of immunosuppression. The reactivated infections usually have lesions that may take 3-5 weeks to heal, a longer period of viral shedding, and are more likely to cause lesions at multiple sites compared to lesions in an immunocompetent host (Pielop et al., 2000). In addition, recurrent infections can result in local or systemic infection, dehydration, and nutritional deficiencies secondary to oral and esophageal lesions. If left untreated, HSV infections can cause severe morbidity and mortality because it is an opportunistic infection in immunocompromised patients. The reactivation rate of HSV among seropositive transplant patients is between 60 and 80% for patients with solid organ transplants and over 80% after bone marrow transplants.
Intravenous acyclovir (5mg/kg every 8 hours for 7 days) is the most commonly used therapy. Penciclovir (PCV) has shown effectiveness to strains that are acyclovir-resistant, a very important benefit seeing as immunocompromised patients sometimes develop resistance to certain antiviral therapies (Lazarus et al., 1999). This occurs as a consequence of injesting many different antiviral therapies for recurrent HSV episodes.
One study (Lazarus
et
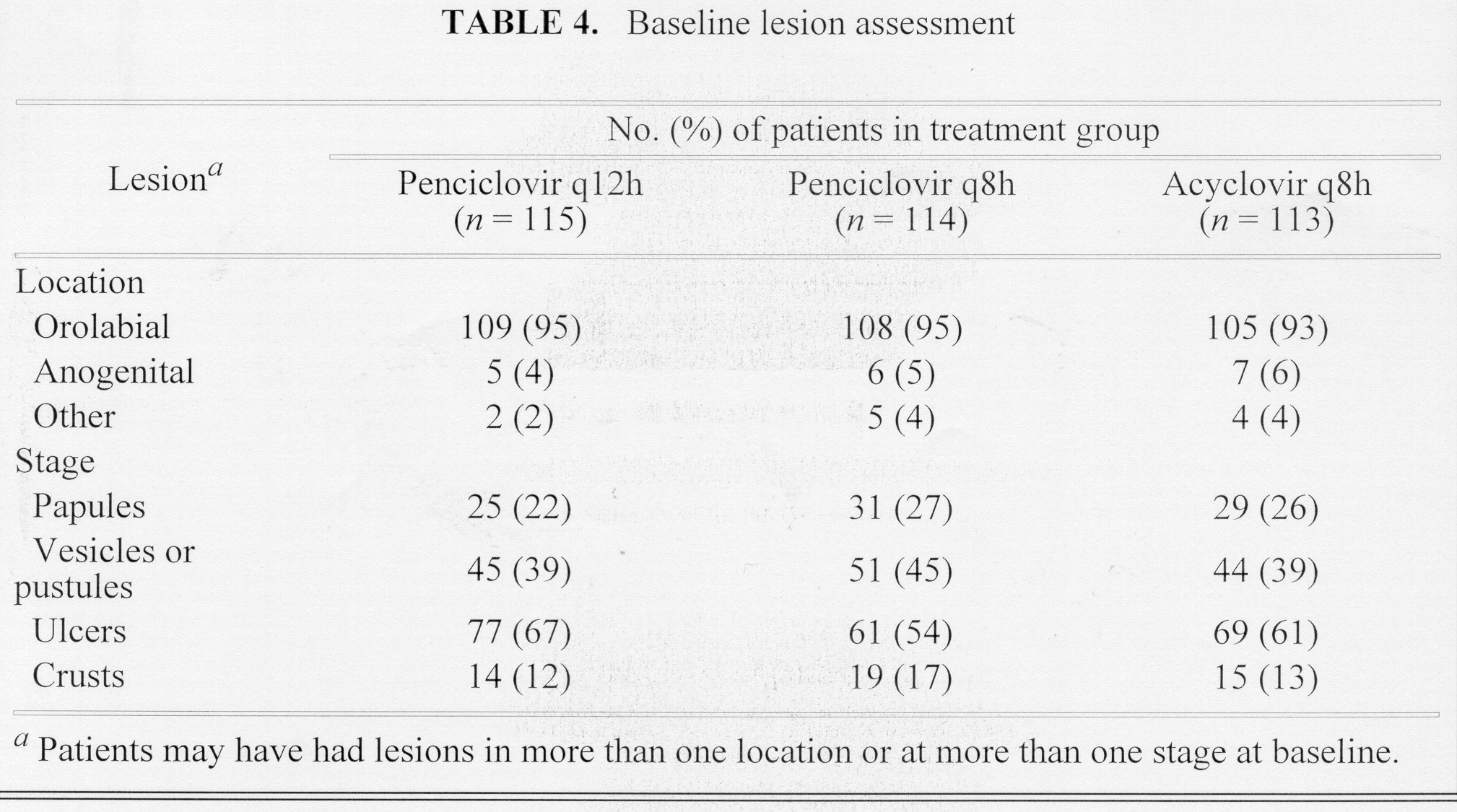
al., 1999) tested the efficacy and safely of penciclovir
(PCV) for the treatment of HSV-1 and HSV-2 infections in immunocompromised
patients while acyclovir was used as the control therapy; primary efficacy
parameter addressed new lesion formation, and secondary addressed viral
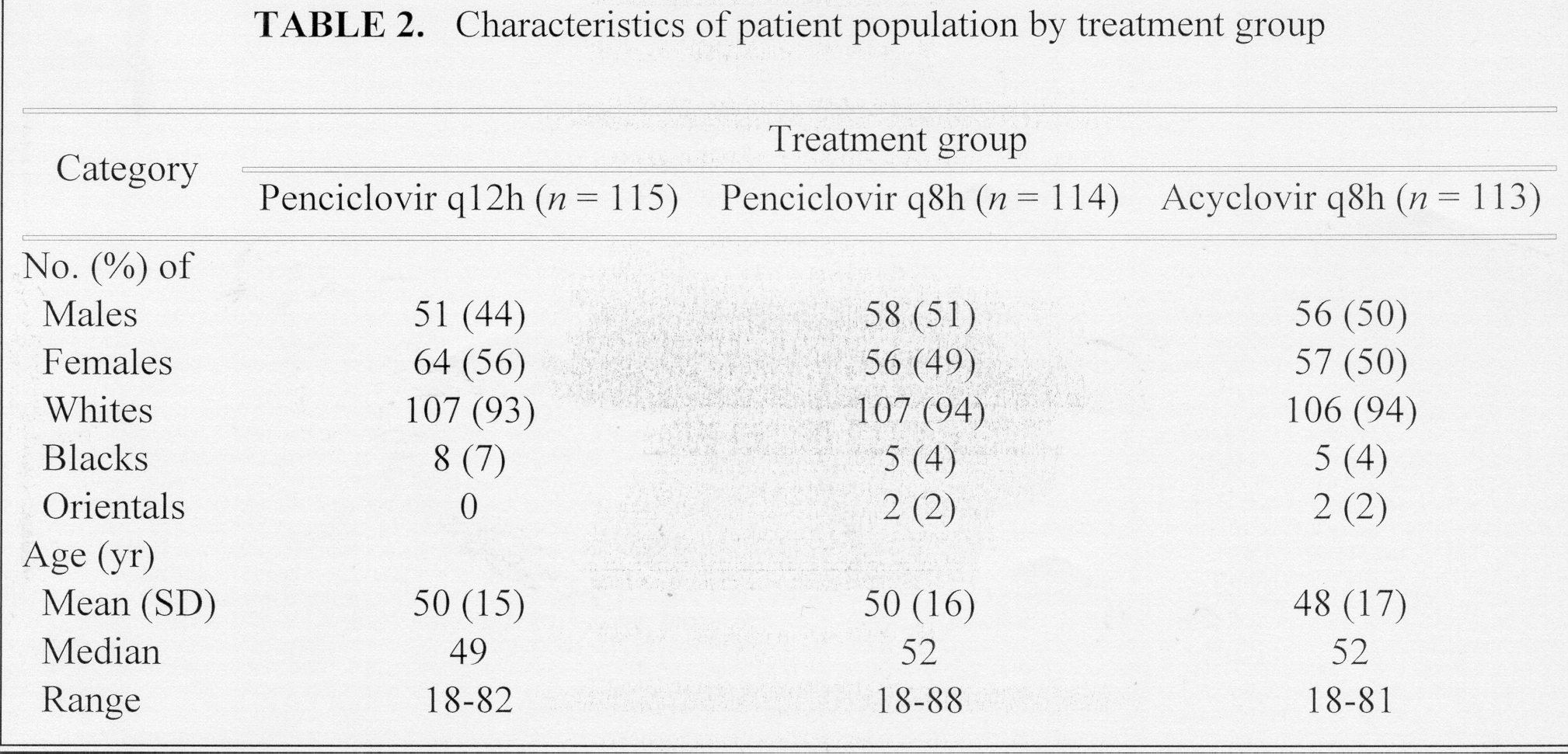
shedding, healing, and pain. Over 300 patients (mean age was 49 years,
94% caucasian, and 52% female) with mucocutaneous HSV infections were tested.
The patients were immunocompromised due to hematologic disorder (63%, including
leukemia, lymphoma, multiple myeloma, myelodysplastic, and aplastic anemia)
and transplant plus hematologic disorder (16%).
 |
 |
Two treatment groups were set up: one was
given 5mg/kg of PCV to take every 12 hours (q12h) and the other was given
5mg/kg of ACV to take every 8 hours (q8h). Known acyclovir-resistant
HSV strains were included in the double-blind assay as controls.
 |
PCV and ACV were well tolerated by all immunocompromised patients with HSV. The results of this study indicate that PCV given every 8 or 12 hours is as safe and effective as ACV for the treatment of HSV in immunocompromised patients. The researchers were extremely satisfied with the fact that the optimum PCV dose is 5mg/kg every 12 hours because the longer duration time makes administering the medication more convenient for the patient (Lazarus et al., 1999).